|
__________
CORRECTION OF THE DYSFUNCTION REVERSES
ALL OF THESE SYMPTOMS
TESTING FOR SIJD
The Passive Straight Leg Raising Test (PSLR)
The PSLR test is commonly used to
test for leg pain and sciatic neuritis. If lifting the straight
leg
causes leg pain that is then increased with dorsiflexion of the
foot (Laseques test) a sciatic neuritis is
indicated. However this test may also be used to determine SIJD.
With SIJD the PSLR test may actually decrease back pain because
the pull on the hamstrings
with PSLR will cause the innominate bone to rotate posteriorly
(backward). PSLR may also increase
pain in the low back on the contra lateral (opposite) side. As
the pelvic bone rotates posteriorly on the
same side it will carry the sacrum back on the opposite innominate
and in effect cause a strain in
anterior rotation on that side.
If PSLR increases pain on the same side (usually the side of the
shorter leg) it is a sign of a
secondary slipping at S1 on that side. This is clinically insignificant
but is treated by many as a posterior
rotation or an upslip. Some chiropractors and PTs mobilize this
joint in an attempt to correct a posterior
dysfunction or an upslip with the patient side-lying, pulling back
on the shoulder and shoving forward and
down on the pelvis. The lumbar spine is already unstable because
of the loose iliolumbar ligaments and
the anterior rotation has overstretched the long posterior ligament.
This incorrect procedure could
tear the annulus, rupture or extrude the disk, tear or avulse the
long posterior ligament and
cause permanent chronic low back pain. THE PRIMARY LESION IS AT
S3 AND THE ONLY
CORRECTION NECESSARY IS OF THE INNOMINATE BONES, BILATERALLY, CEPHALAD
AT
S1 AND CAUDAD AND MEDIALLY ON THE SACRUM AT S3.
Leg Shortening Test
As the dysfunction in anterior rotation always causes the legs
to get longer, sometimes one more
than the other, a manual rotation of the innominate bones on the
sacrum will cause each leg to appear to
get shorter. This shortening of an apparent long leg is a positive
sign that has the advantage of correcting
the dysfunction.
First stand at the foot of the plinth, grasp both ankles holding
a thumb immediately caudad to each
medial malleolus (ankle bone) and approximate the ankles in the
mid-line. Check the leg length. Now
it does not matter if the leg length appears to be even, or longer
on the more painful side or shorter on
the more painful side. Lift either leg to about 45 degrees of PSLR
and traction it in the long axis hard
enough to lift the buttock on that side. This will cause the PSIS
to move caudad on the sacrum. If
dysfunction is present, each leg will get shorter with flexion
of each innominate on the sacrum. If they are
even, one leg will about 1cm shorter after testing. If you pull
on the long leg, the legs will probably appear to
be of equal length. If you pull on the short leg at about 45 degrees
of PSLR, it will appear to get shorter and
may appear to be from 1-3 cm shorter than the other.
Continue correcting with various described corrections gradually
increasing pressure in posterior
innominate rotation. Do not stop when the legs appear to be of
equal length, but only after the legs
no longer appear to get any shorter.
Injections
The primary points of pain are at the PSIS
and PIIS and are extra-articular. If there are no tears
in the capsule the injection will become encapsulated and a diagnostic
injection may give a false negative
result. Murakami et al (J Ortho Science May 2007) in comparing
periarticular and intraarticular
injections for sacroiliac joint pain injected periarticular lidocaine
in 25 consecutive patients with SIJD
and found that it was effective in ALL patients. Intraarticular
injections were effective in 9 of 25 patients.
An additional 16 patients who had no relief from the initial intraarticular
injection were ALL relieved
from a periarticular injection.
back to top
__________
X-rays
In 1978 Davis and Lentle used technitium 99M stannous pyrophosphate
bone scanning with
quantitative sacroiliac scintigraphy in 50 female patients with
LBPS. They reported that 22 patients
(44%) had sacroiliitis. Eight of these (36%) had unilateral sacroiliitis
and 14 (64) had bilateral
sacroiliitis. Of the 22 patients with abnormal scans, 20 had normal
radiographs
(Lancet 2:496-497, 1978)
Conventional X-rays will not demonstrate this dysfunction thus
complicating conventional evaluation and treatment. Referrals to psychiatrists are not helpful and the
patient frequently seeks
unconventional care. Scanning of the lumbar spine does not usually include
the SIJs. When scanning,
look for longitudinal tearing in the piriformis muscle at the posterior inferior
iliac spine. Arthrography
of the SIJ may demonstrate tears in the capsules, especially at or near the
PIIS.

click
to enlarge

click
to enlarge
Roentgenograms taken before (Above) and after (Below) correction
of SIJD reveal a dysfunction of
the innominate bone cephalad and laterally on the sacrum. Note movement
of the PSISs relative to
the sacral foramina.
Incidence
Shaw did a study of 1000 consecutive cases of idiopathic low back pain. Using
objective
changes in leg length and changes in the pelvis from asymmetry to symmetry
as guides he found
an incidence of 98% with SIJD contributing. His surgical incidence for herniated
disk dropped
to 0.2%. (Reported in First World Congress on Low Back Pain and the Sacroiliac
Joint 1992)
back to top
__________
Corrective Exercises
Clinical Basis for Treatment
As with the subluxation/dislocation of any joint, the first priority is to
reduce the subluxation.
If it tends to recur the patient can be taught to self-correct. If the lesion
is unstable, a lumbosacral
support or invasive procedures may be necessary.
Dysfunction of the sacroiliac joint is essentially always a pathological release
of the balanced
position with an anterior rotation of the innominate bones on the sacrum. Treatment
is simply restoring
the innominates back to the balanced position. It does not matter if one leg
appears to be longer or
shorter on the more painful side of if they appear to be of equal length, they
will each always appear to
shorten with correction of the SIJ to the balanced position. If there is no
history of a congenital leg
length difference, polio or serious leg fracture the legs will appear to be
of equal length after correction.
The corrections should be done every 2-3 hours all day long for at least three
days to take the
tension off of the tight ligaments and give them an opportunity to recover.
After that correct at any sign
of recurrence.
Nature of the Correction
The corrective procedure is not a vertebral manipulation. No high or low speed
manipulative
thrust is necessary or indicated. No jerking or popping is necessary or desirable.
Correction is
achieved by specifically applied traction on the properly positioned joint
or by a precise manual rotation
of the innominate bones posteriorly on the sacrum.
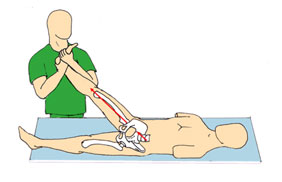
Manual Correction of the S3 Subluxation
Any of several methods can be used to restore the SIJ to the balanced position:
traction at
about 45 degrees of PSLR; direct posterior rotation of the innominates on the
sacrum; or by using
isometric or muscle energy techniques.
 |
|
 |
Traction must be strong enough
to lift the buttock on that side and
held for several seconds.
When distracting the leg have the patient lift his/her
head and tighten the abdominal muscles to
enhance the posterior pelvic rotation.
First do one side and then the other, checking the leg length
at the malleoli and watch for
shortening. Do each leg, one at a time 4-5 times on each side, alternating
sides each time and
checking leg length each time. The movement of the PSIS caudad on the sacrum
can be palpated.
Do not pull on the leg in a direct line with the body.
back to top
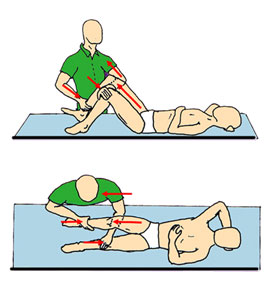
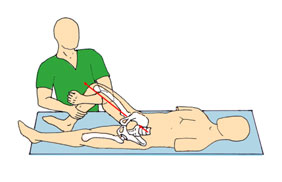
THE EZ FIX
For a correction on the right side, put your left forearm under
the right knee and your left hand over the front of the left
knee. Push off with your left foot to provide traction, pulling
on the leg with the left forearm. The left hand will help
to lever the traction. Put just enough force on the right
ankle with your right hand to hold the knee in flexion. Apply
enough traction to lift the buttock on that side. Do each
side 3-4 times, alternating sides each time. To enhance the
correction have the patient lift his/her head to tighten
the abdominal muscles. The tight SIJ acts like a stuck drawer
and gives just a little bit at a time on each side.
|
|
|
|
|
|
|
|
|
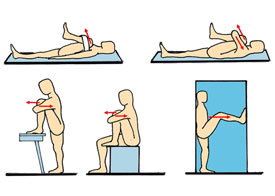
SELF-TRACTION SUPINE
The patient can use traction for self-correction by pushing
the thigh toward the foot hard enough to lift the buttock
on that side. Lifting the head at the same time will enlist
the abdominal muscles. Repeat several times on each side
alternating sides each time.
Do especially when you go to bed a night.
|
|
 |
|
|
|
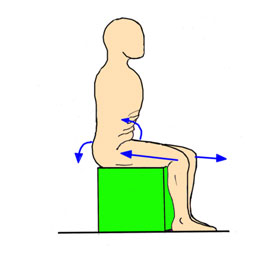
SEATED
PATIENT CORRECTION may be done while
at a desk or in a car. Push one knee out. Pull the other
knee back firmly to pull the pelvis down in back. Tighten
your abdominal
muscles to pull
the pelvis up in front. Do several times on each side alternating
each time. Repeat several times daily.
|
|
 |
|
|
|
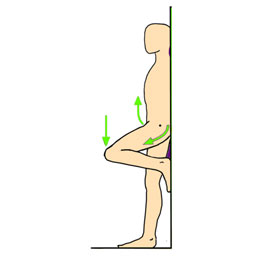
STANDING PATIENT CORRECTION
Tighten abdominal
muscles and push the knee toward the floor. Repeat on the other
side. Alternate exercise several times on each side. Repeat
correction several times during the day. |
|
 |
|
|
|
|
|
|
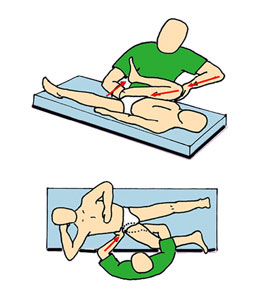
DIRECT
CORRECTION (Two methods)
1. In the direct correction the leg can be used as a lever
and brought to the outside of the body. Knee to axilla. Put
one hand under the ischial tuberosity and the other on the
top of the patient's knee. While lifting with the lower hand,
push downward on the shaft of the femur while also rotating
the thigh into flexion.
2. The operator can also directly rotate the pelvis posteriorly
by placing one hand under the ischial tuberosity and the other
over the posterior aspect of the iliac crest. Rotate firmly
pushing with the thenar eminence.
|
|
 |
|
|
|
|
|
|
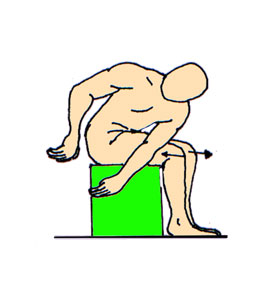
DIRECT PATIENT CORRECTION
The patient can self-correct any time during the day no matter
what position he happens to be in at the time. Just by pulling
the knee into the axilla or bringing the axilla down to the
knee. Stretch firmly several times on each side, alternating
sides each time.
When doing any of these exercises in the supine position be certain to hold your
abdominal muscles tight when raising or lowering your leg to prevent anterior
rotation of the pelvis.
|
|
 |
|
|
|
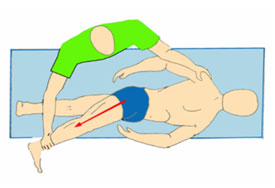
FLANK STRETCH
Following the direct correction a stretch of the quadratus
lumborum and the hip abductors can be helpful in achieving
further correction.
Stretch gently as indicated then have patient lift
his leg against resistance and then relax.
Take up the slack and put traction on the leg as indicated.
This may necessitate the aid of an assistant. Follow this
with a hard isometric
correction. |
|
 |
|
|
|
ISOMETRIC CORRECTION
Grasp the knee with both arms, hold firmly and push very hard
outward with the knee. Be sure to tighten the abdominal muscles
while pushing with the knee to enhance posterior rotation
of the pelvis and when lowering your leg.
A six-foot luggage belt may be used for resistance or the patient
can stand in a door frame and push as shown. This is a very
powerful correction. Push hard and hold for several seconds
each time. |
|
 |
|
|
|
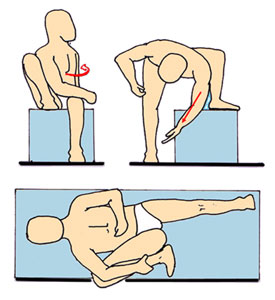
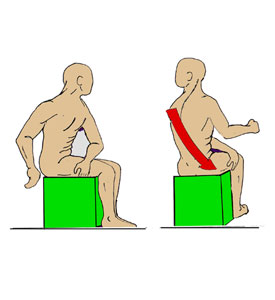
STRETCHING THE CORE MUSCLES ON THE ASYMMETRIC
PELVIS
As the core muscles are most active during normal gait when
the pelvis is asymmetrical, they are most effectively stretched
when the pelvis is asymmetrical. Seated, project one thigh
and retract the other to create an asymmetric pelvis. Flex
and twist your trunk toward the side of the retracted thigh.
This stretches the piriformis, the sacral origin of the gluteus
maximus, the quadratus lumborum, the multifidus, the abdominal
obliques, the latissimus dorsi and others. Repeat toward the
other side.
ALWAYS DO CORRECTIVE EXERCISES BEFORE AND AFTER THESE STRETCHES.
|
|
 |
|
|
|
STRENGTHENING THE CORE ON THE ASYMMETRIC
PELVIS USING MUSCLE ENERGY TECHNIQUES
In order to strengthen the same muscle groups, retract your
right thigh and project your left. Twist trunk to the left
and grasp the right leg with the left hand. Now extend and
rotate the trunk to the left while projecting the right thigh
and retracting the left. Provide resistance to the trunk rotation
with the left hand. Repeat on other side.
|
|
 |
|
|
|
MUSCLE ENERGY EXERCISE FOR THE CORE ON THE
SYMMETRICAL PELVIS
Strengthening the rectus abdominis and the abdominal oblique
musculature is necessary to help maintain posterior pelvic
rotation throughout the day. This exercise is done on the symmetrical
pelvis. Place both hands on the same knee, tighten your abs
and pinch your buttocks tightly together. Push down hard on
that knee for several seconds. Repeat on the other side. Do
five times on each side.
Repeat throughout the day.
|
|
 |
ACTIVE EXERCISE FOR THE CORE,
GLUTES AND THIGHS
Seated, simply tighten your abs and glutes, hold tight, lean forward
and rise to standing, slowly. Then, still holding your abs and
glutes tightly, sit slowly. Repeat ten times.
Always tighten your abdominal muscles when standing and sitting.
back to top
__________
Medical Management
Sequence (Non-invasive)
Correct the joint, instruct patient in self-correction and tell
him to do the corrective exercises every
two to three hours all day long for the next three days at least
in order to keep the tension off of the
affected ligaments and allow them to recover.
On the second day have the patient demonstrate the corrective exercises
to you. They will
usually be making errors in technique that will preclude a good
result and must be re-instructed.
If the patient is doing the exercises properly he/she should be
told to only return if the pain continues
over 10 days.
If the pain still recurs after ten days the patient should be put
into a lumbosacral support.
This support is to be put on when lying down on it and after making
a correction. If progress continues
with the support the patient can wean himself as indicated.
If the dysfunction is still unstable after one month, proliferant
injections are indicated into the long
and short posterior sacroiliac ligaments. These are the only ligaments
so affected.
Contraindications
Contraindications are few.
• Do not stretch a tight psoas. Correction will restore normal
tension in the psoas.
• No double or single straight leg raising.
• No sit-ups with the legs out straight.
• Never correct into pain. If what you are doing causes pain
use a different correction.
Hip fractures or hip replacements are not contra indications.
Just change to a direct correction by
grasping the pelvis directly without using the leg as a lever.
• Never prolo the iliolumbar ligaments until the SIJ is corrected
and stable. This may preclude the
possibility of achieving correction.
• Never correct for a posterior dysfunction or an upslip. This
correction is unsafe and potentially harmful.
Invasive Methods
Invasive procedures may be necessary if conservative measures
fail. Begin with the least
invasive measures first:
Local Anesthetic
Periarticular injections of local anesthetic and steroid to
the area of the posterior inferior Iliac
spine and the posterior superior iliac spine to relieve acute
pain and inflammation.
Proliferant injections
Proliferant injections to the long and short posterior sacroiliac
ligament to stabilize the joint.
Do not proliferate any other ligaments until the joint is stable or you might
tighten the joint in the
uncorrected position and preclude the possibility of correction. Always proliferate
with the SIJ in the
corrected position of posterior innominate rotation.
There may be some value in proliferating the long
and short posterior sacroiliac ligaments in
the early stages of low back pain. This might strengthen those ligaments
to limit collagen failure, help
to prevent recurrence of dysfunction and preserve the system. If ligamentous
balance is not maintained
the collagen may still fail in the long posterior sacroiliac ligament even
if it has been proliferated.
Stability of the lower lumbar vertebra
is restored with correction and stabilization of the
sacroiliac joint. If after the sacroiliac joints are stabilized in the
balanced position the iliolumbar
ligaments may be proliferated if they are still unstable.
The Failed Back
In the patient with multiple fusions and a failed back, in the likely event
of an unstable SIJ,
it is probably critical to preserve function with ligamentous repair rather
than stabilize. The importance
of these joint to absorb, modify and redirect the various forces that occur
during normal gait can not
be overstated. Excess rigidity will predispose to systems failures.
Failed prolo
Prolo may not be effective if:
1. The superficial long posterior sacroiliac ligament has undergone extreme
visco
elastic failure.
2 The ligament is shredded or otherwise traumatized.
3. The ligament is not in a corrected and shortened position when injected.
4. If the ligament is avulsed from its attachment to the PSIS.
5. If the patient has a protruding abdomen and refuses to lose weight.
Ligamentous Repair
If it is not possible to stabilize the joint with proliferant then you
might consider ligamentous
repair of the long posterior SI ligament. It is superficial and quite accessible.
It may be feasible to
transfer tendon from the adjacent sacrospinalis muscle to the PSIS and
marry it with proliferant to
the long posterior SI ligament. Always operate with the joint in the corrected
position.
Surgical Fixation
In the event of severe joint injury and gross ligamentous instability surgical
fixation may be
necessary. Fixate in the corrected position. Caution the patient as to
limiting activities that create
or increase the asymmetric pelvis. If these activities are blocked posteriorly
they will manifest
anteriorly and destabilize the symphysis.
After fixation, if the patient uses a non-weight bearing gait, the ipsilateral
leg hanging down
from the innominate bone will cause a force in anterior rotation on the
pelvis and might cause a
non-union to occur.
The Epidural
An epidural anesthetic may relieve the pain of SIJD because of the lumbar
innervation of the
SIJs, however this should not be interpreted as relief of a referred pain
of lumbar origin. It is more
effective to treat locally to relieve pain and inflammation.
The Piriformis Release
If correcting the SIJ does not relieve the pain or if the patient has an
SIJ fixation in the
uncorrected position, consider releasing only the secondary origin of the
piriformis from the roof of
the greater sciatic notch to preserve function in that muscle. Cutting
the tendon of the piriformis
muscle decreases sacral stability during ambulation.
__________
Note to Physicians
When ordering therapy please specify the DonTigny Method. Many therapists
are still using
methods based on standard AAOS testing or are using traditional side-lying
manipulations.
Richard L. DonTigny passed away March 15, 2023. Please download and share the links below. Much of his work is also on ResearchGate.
----
PELVIC DYNAMICS FOR THE PROFESSIONAL........................$0.00 (US Funds)
Includes:
Pelvic Dynamics Pro Program - 22MB PDF with 650 slides and 150 illustrations
18-minute video, 180MG mpg download with demonstration of corrective exercises
Dynamic Core Program - 3MB PDF
FAQs - 5MB pdf
Complete description of disc contents
This work is the result of 38 years of clinical practice, about
8000 cases of SIJD and 40 years of research.
This program is offered as a public service.
back to top
|